

Volume 11, Issue 1 (March 2026)
J Environ Health Sustain Dev 2026, 11(1): 2904-2914 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Nikseresht L, Dowlatabadi A, Nasab H, Alimohammadi Ardakani M, Mokhtari M. Strategies for Minimizing Health Care Waste: A Systematic Review Study. J Environ Health Sustain Dev 2026; 11 (1) :2904-2914
URL: http://jehsd.ssu.ac.ir/article-1-1007-en.html
URL: http://jehsd.ssu.ac.ir/article-1-1007-en.html
Leili Nikseresht 

 , Afshin Dowlatabadi , Habibeh Nasab , Majid Alimohammadi Ardakani , Mehdi Mokhtari *
, Afshin Dowlatabadi , Habibeh Nasab , Majid Alimohammadi Ardakani , Mehdi Mokhtari *
, Afshin Dowlatabadi , Habibeh Nasab , Majid Alimohammadi Ardakani , Mehdi Mokhtari *
Environmental Sciences and Technology Research Center, Department of Environmental Health Engineering, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Full-Text [PDF 540 kb]
(179 Downloads)
| Abstract (HTML) (786 Views)
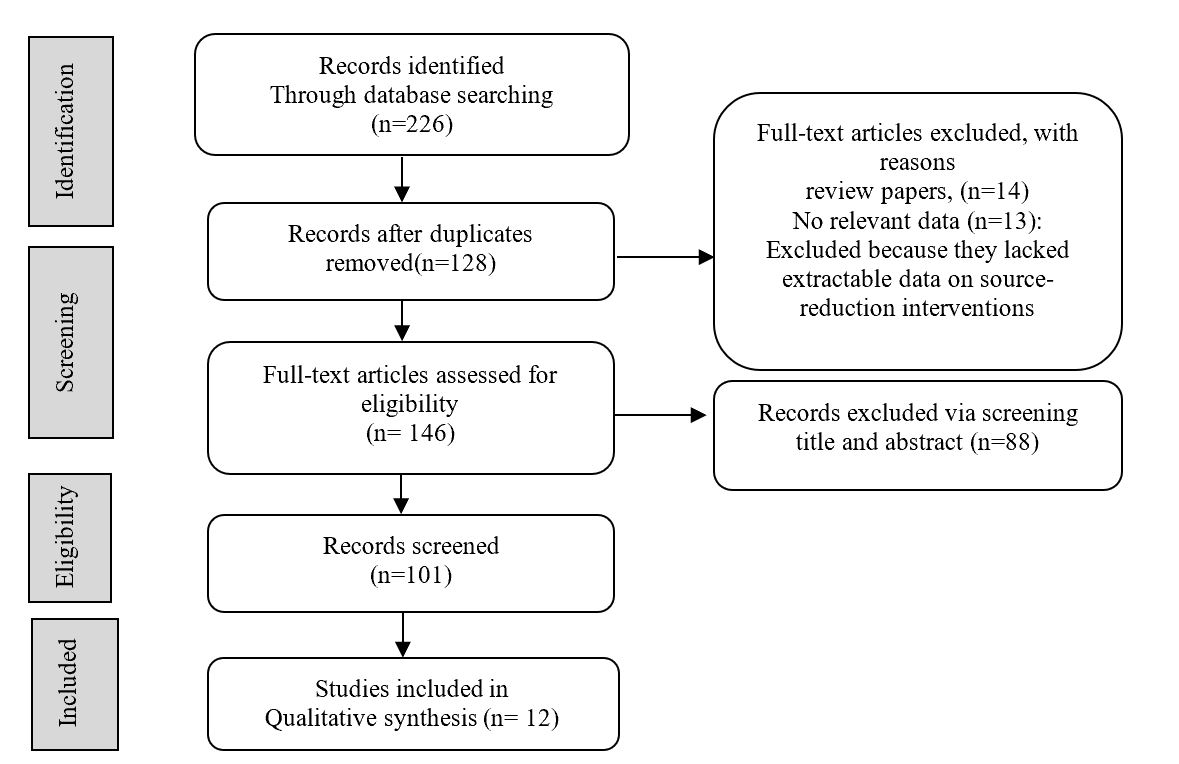
Table 1: Quality Assessment of Included Studies
Table 2: Characteristics and Key Findings of Included Studies on Health Care Waste Minimization Strategies
Full-Text: (34 Views)
Strategies for Minimizing Health Care Waste: A Systematic Review Study
Leili Nikseresht 1, Afshin Dowlatabadi 1, Habibeh Nasab 1, Majid Alimohammadi Ardakani 2 ,Mehdi Mokhtari 1*
1 Environmental Sciences and Technology Research Center, Department of Environmental Health Engineering, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Department of Industrial Engineering , Faculty of Engineering, Ardakan University, Ardakan, Iran.
Leili Nikseresht 1, Afshin Dowlatabadi 1, Habibeh Nasab 1, Majid Alimohammadi Ardakani 2 ,Mehdi Mokhtari 1*
1 Environmental Sciences and Technology Research Center, Department of Environmental Health Engineering, School of Public Health, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2 Department of Industrial Engineering , Faculty of Engineering, Ardakan University, Ardakan, Iran.
| A R T I C L E I N F O | ABSTRACT | |
| SYSTEMATIC REVIEW | Introduction: Solid waste from healthcare centers is a major health and environmental challenge that imposes significant costs on the healthcare system. Methods: This systematic review was conducted following the PRISMA guidelines. A comprehensive search was conducted in the PubMed, Scopus, and Web of Science databases using keywords related to healthcare waste reduction, and Google Scholar was used as a supplementary source. Original quantitative, qualitative, and mixed-method studies examining waste reduction interventions in healthcare settings were included. The quality of the studies was assessed using the Newcastle Ottawa scale, and only studies with moderate to high quality were included in the final synthesis of results. The data were analyzed narratively and descriptively. Results: Twelve studies were included in the review. The results showed that educational and management interventions, such as implementing comprehensive quality management models, pharmaceutical interventions, such as prescription review, use of multi-dose vials, and rounding of drug doses, as well as redesigning hospital nutrition services and employing safe technologies and alternatives, resulted in significant waste reduction and cost savings. Among these, pharmacy bundles and targeted staff training were the most effective interventions. Conclusion: This review found that various strategies have been used to reduce healthcare waste in different countries, with pharmaceutical packaging optimization and educational programs showing the greatest effectiveness. However, there is still a need for larger intervention studies and evaluations of long-term clinical and economic outcomes. |
|
Article History: Received: 23 October 2025 Accepted: 20 January 2026 |
||
*Corresponding Author: Mehdi Mokhtari Email: mhimokhtari@gmail.com Tel: +98 35 31492270 |
||
Keywords: Waste Managements; Medical Waste; Environmental Pollution. |
Citation: Nikseresht L, Dowlatabadi A, Nasab H, et al. Strategies for Minimizing Health Care Waste: A Systematic Review Study. J Environ Health Sustain Dev. 2026; 11(1): 2904-14.
Introduction
One of the increasing challenges in public health is the effective management of waste generated by healthcare services. Healthcare waste (HCW) includes a diverse array of materials produced during diagnostic, therapeutic, caregiving, research, and educational activities in hospitals, laboratories, and clinics 1. Based on their nature, these wastes are generally divided into two main categories: non-hazardous waste (approximately 75–85%) and hazardous waste (15–25%), which includes infectious, chemical, pharmaceutical, radioactive, and sharp waste. Inadequate management of such waste poses serious risks to patients, healthcare workers, the community, and the environment 2, 3.
Factors such as population growth, expansion of healthcare facilities, advances in medical technology, and increased use of disposable equipment and pharmaceuticals have led to a continuous increase in the volume of medical waste 4. According to international reports, the average generation of medical waste in hospitals ranges from 0.5 to 3 kg per bed per day, with healthcare facilities in developing countries often exceeding international standards 5. In many cases, improper segregation and insufficient awareness among healthcare personnel result in non-hazardous waste being incorrectly classified as hazardous, thereby increasing disposal costs and environmental impact 6.
Given the far-reaching consequences of medical waste on public health, occupational safety, healthcare costs, and the environment, the adoption of strategies for waste minimization at the source and enhancement of waste management practices within health systems have become increasingly critical 7. Waste minimization refers to reducing waste generation, improving resource efficiency, recycling reusable materials, and adopting safer and environmentally friendly alternatives in healthcare. These measures not only reduce the direct costs of waste disposal but also minimize the risks of infection transmission, environmental pollution, and exposure of healthcare staff to hazardous agents 8.
Various studies have explored strategies for minimizing healthcare waste 9. These strategies include proper waste segregation at the point of generation, staff education and empowerment, the use of cleaner technologies, rational planning for drug and food consumption, reducing the frequency of injectable drug preparation, redesigning clinical processes, substituting hazardous substances with safer alternatives, and implementing quality management systems such as TQM or Lean Six Sigma. Some of these interventions have been applied at the hospital level and have demonstrated significant reductions in both waste volume and management costs 10. However, despite remarkable progress in healthcare waste management, the lack of a comprehensive and systematic review of existing evidence on waste minimization strategies across different levels of healthcare services has resulted in fragmented information and limited practical guidance for policymakers and hospital managers 10.
In contrast to previous reviews that broadly addressed healthcare waste management systems, the present study is distinguished by its specific focus on waste minimization at the source, within clinical service environments. To the best of our knowledge, this is the first systematic review to highlight and synthesize evidence on pharmacy bundles (including dose rounding, vial optimization, batching frequency, and pharmacist-led review) and hospital food-service redesign as high-impact strategies for reducing healthcare waste. The methodological quality of the included studies was assessed using the standardized Newcastle Ottawa Scale (NOS), and studies published up to 2025 were incorporated to ensure comprehensive and up-to-date coverage. Through this approach, a timely, evidence-based, and operational synthesis was developed to support hospitals and policymakers in advancing waste reduction practices beyond traditional segregation methods. Therefore, this study aimed to systematically review the published evidence on strategies to minimize healthcare waste, categorize intervention types, evaluate their outcomes, and identify existing gaps to support informed decision-making and policy development.
Materials and Methods
This study followed the PRISMA guidelines for systematic reviews; however, owing to the heterogeneity among the included studies, a meta-analysis was not conducted 11.
Search Strategy
A comprehensive and systematic search was conducted to identify relevant studies on strategies for healthcare waste minimization published between January 2000 and March 2025. Searches were performed in PubMed, Scopus, and the Web of Science. Google Scholar was used as a supplementary source to identify potentially missed studies. The search strategy combined controlled vocabulary and free-text terms, including “healthcare waste,” “healthcare solid waste,” “biomedical waste,” “waste minimization,” “waste reduction,” “waste prevention,” “clean technology,” “interventions,” “waste segregation in healthcare,” “sharps waste management,” and “strategy.” The reference lists of the included studies were manually screened using a snowballing technique. Non-English studies were included only when full-text translations were available.
Study Selection
This review focused on strategies to minimize healthcare waste at the source within clinical service environments. The scope included six waste categories: clinical/infectious, pharmaceutical, chemical, radioactive, sharps, and food service waste. Eligible studies were conducted in healthcare delivery settings, such as hospitals, clinics, dialysis centers, and ambulatory surgical centers. Original quantitative, qualitative, or mixed-method studies were included if they evaluated at least one intervention designed to reduce waste generation or improve resource efficiency, segregation, or cost outcomes. Studies were excluded if they addressed non-medical or municipal waste streams, lacked an intervention component, or were review articles, editorials, letters, conference abstracts, or studies with insufficient or non-extractable data. A PRISMA flow diagram summarizes the selection process, including the reasons for exclusion at the full-text review stage (Figure. 1).
Data Extraction
Data extraction was performed independently by two reviewers using a predefined template to ensure consistency of the results. The extracted items included study author, year, country, healthcare setting, study design, sample characteristics (where applicable), waste type and source, intervention description, implementation requirements, outcomes (e.g., change in waste volume, cost, segregation quality, resource efficiency), reported implementation barriers and study limitations. Any discrepancies were resolved through discussion, and unresolved conflicts were adjudicated by a third reviewer if necessary.
Because the included studies varied substantially in terms of design, intervention structure, outcome definitions, measurement tools, and reporting formats, statistical pooling was not feasible. Therefore, we used a narrative synthesis approach to summarize the findings across four predefined domains. This method allowed us to account for heterogeneity and highlight convergent evidence while preserving the contextual details across studies.
Quality Assessment
The methodological quality and risk of bias for the included observational and interventional studies were assessed using the Newcastle–Ottawa Scale (NOS), which evaluates three domains: (1) selection of participants, (2) comparability of study groups, and (3) measurement of outcome/exposure. Each study was scored between 0 and 9. Two reviewers independently performed the assessments, and discrepancies were resolved through discussion. All included studies scored between 7 and 9, indicating moderate to high methodological quality; therefore, none were excluded for insufficient quality.
Data combination
Owing to heterogeneity in study design, intervention type, and outcome measures, a narrative synthesis approach was used. The findings were categorized into four intervention categories: educational and management interventions, pharmaceutical interventions, hospital nutritional interventions, and technological and environmental interventions. The results are presented descriptively in tables, including study characteristics, quality assessment, interventions, and outcomes; no meta-analysis was performed 12.
Results
A total of 226 records were identified through database searches. After removing 98 duplicates, 128 records remained for further screening. Of these, 14 review articles and 13 studies with incomplete data were excluded from the analysis. The full texts of 101 articles were then assessed for eligibility, and 88 were excluded because they primarily focused on post-generation waste segregation rather than on source-minimization strategies. Ultimately, 13 studies met the inclusion criteria and were included in this systematic review (Figure. 1).
One of the increasing challenges in public health is the effective management of waste generated by healthcare services. Healthcare waste (HCW) includes a diverse array of materials produced during diagnostic, therapeutic, caregiving, research, and educational activities in hospitals, laboratories, and clinics 1. Based on their nature, these wastes are generally divided into two main categories: non-hazardous waste (approximately 75–85%) and hazardous waste (15–25%), which includes infectious, chemical, pharmaceutical, radioactive, and sharp waste. Inadequate management of such waste poses serious risks to patients, healthcare workers, the community, and the environment 2, 3.
Factors such as population growth, expansion of healthcare facilities, advances in medical technology, and increased use of disposable equipment and pharmaceuticals have led to a continuous increase in the volume of medical waste 4. According to international reports, the average generation of medical waste in hospitals ranges from 0.5 to 3 kg per bed per day, with healthcare facilities in developing countries often exceeding international standards 5. In many cases, improper segregation and insufficient awareness among healthcare personnel result in non-hazardous waste being incorrectly classified as hazardous, thereby increasing disposal costs and environmental impact 6.
Given the far-reaching consequences of medical waste on public health, occupational safety, healthcare costs, and the environment, the adoption of strategies for waste minimization at the source and enhancement of waste management practices within health systems have become increasingly critical 7. Waste minimization refers to reducing waste generation, improving resource efficiency, recycling reusable materials, and adopting safer and environmentally friendly alternatives in healthcare. These measures not only reduce the direct costs of waste disposal but also minimize the risks of infection transmission, environmental pollution, and exposure of healthcare staff to hazardous agents 8.
Various studies have explored strategies for minimizing healthcare waste 9. These strategies include proper waste segregation at the point of generation, staff education and empowerment, the use of cleaner technologies, rational planning for drug and food consumption, reducing the frequency of injectable drug preparation, redesigning clinical processes, substituting hazardous substances with safer alternatives, and implementing quality management systems such as TQM or Lean Six Sigma. Some of these interventions have been applied at the hospital level and have demonstrated significant reductions in both waste volume and management costs 10. However, despite remarkable progress in healthcare waste management, the lack of a comprehensive and systematic review of existing evidence on waste minimization strategies across different levels of healthcare services has resulted in fragmented information and limited practical guidance for policymakers and hospital managers 10.
In contrast to previous reviews that broadly addressed healthcare waste management systems, the present study is distinguished by its specific focus on waste minimization at the source, within clinical service environments. To the best of our knowledge, this is the first systematic review to highlight and synthesize evidence on pharmacy bundles (including dose rounding, vial optimization, batching frequency, and pharmacist-led review) and hospital food-service redesign as high-impact strategies for reducing healthcare waste. The methodological quality of the included studies was assessed using the standardized Newcastle Ottawa Scale (NOS), and studies published up to 2025 were incorporated to ensure comprehensive and up-to-date coverage. Through this approach, a timely, evidence-based, and operational synthesis was developed to support hospitals and policymakers in advancing waste reduction practices beyond traditional segregation methods. Therefore, this study aimed to systematically review the published evidence on strategies to minimize healthcare waste, categorize intervention types, evaluate their outcomes, and identify existing gaps to support informed decision-making and policy development.
Materials and Methods
This study followed the PRISMA guidelines for systematic reviews; however, owing to the heterogeneity among the included studies, a meta-analysis was not conducted 11.
Search Strategy
A comprehensive and systematic search was conducted to identify relevant studies on strategies for healthcare waste minimization published between January 2000 and March 2025. Searches were performed in PubMed, Scopus, and the Web of Science. Google Scholar was used as a supplementary source to identify potentially missed studies. The search strategy combined controlled vocabulary and free-text terms, including “healthcare waste,” “healthcare solid waste,” “biomedical waste,” “waste minimization,” “waste reduction,” “waste prevention,” “clean technology,” “interventions,” “waste segregation in healthcare,” “sharps waste management,” and “strategy.” The reference lists of the included studies were manually screened using a snowballing technique. Non-English studies were included only when full-text translations were available.
Study Selection
This review focused on strategies to minimize healthcare waste at the source within clinical service environments. The scope included six waste categories: clinical/infectious, pharmaceutical, chemical, radioactive, sharps, and food service waste. Eligible studies were conducted in healthcare delivery settings, such as hospitals, clinics, dialysis centers, and ambulatory surgical centers. Original quantitative, qualitative, or mixed-method studies were included if they evaluated at least one intervention designed to reduce waste generation or improve resource efficiency, segregation, or cost outcomes. Studies were excluded if they addressed non-medical or municipal waste streams, lacked an intervention component, or were review articles, editorials, letters, conference abstracts, or studies with insufficient or non-extractable data. A PRISMA flow diagram summarizes the selection process, including the reasons for exclusion at the full-text review stage (Figure. 1).
Data Extraction
Data extraction was performed independently by two reviewers using a predefined template to ensure consistency of the results. The extracted items included study author, year, country, healthcare setting, study design, sample characteristics (where applicable), waste type and source, intervention description, implementation requirements, outcomes (e.g., change in waste volume, cost, segregation quality, resource efficiency), reported implementation barriers and study limitations. Any discrepancies were resolved through discussion, and unresolved conflicts were adjudicated by a third reviewer if necessary.
Because the included studies varied substantially in terms of design, intervention structure, outcome definitions, measurement tools, and reporting formats, statistical pooling was not feasible. Therefore, we used a narrative synthesis approach to summarize the findings across four predefined domains. This method allowed us to account for heterogeneity and highlight convergent evidence while preserving the contextual details across studies.
Quality Assessment
The methodological quality and risk of bias for the included observational and interventional studies were assessed using the Newcastle–Ottawa Scale (NOS), which evaluates three domains: (1) selection of participants, (2) comparability of study groups, and (3) measurement of outcome/exposure. Each study was scored between 0 and 9. Two reviewers independently performed the assessments, and discrepancies were resolved through discussion. All included studies scored between 7 and 9, indicating moderate to high methodological quality; therefore, none were excluded for insufficient quality.
Data combination
Owing to heterogeneity in study design, intervention type, and outcome measures, a narrative synthesis approach was used. The findings were categorized into four intervention categories: educational and management interventions, pharmaceutical interventions, hospital nutritional interventions, and technological and environmental interventions. The results are presented descriptively in tables, including study characteristics, quality assessment, interventions, and outcomes; no meta-analysis was performed 12.
Results
A total of 226 records were identified through database searches. After removing 98 duplicates, 128 records remained for further screening. Of these, 14 review articles and 13 studies with incomplete data were excluded from the analysis. The full texts of 101 articles were then assessed for eligibility, and 88 were excluded because they primarily focused on post-generation waste segregation rather than on source-minimization strategies. Ultimately, 13 studies met the inclusion criteria and were included in this systematic review (Figure. 1).
Table 1 summarizes the quality assessment results of the 13 studies. Overall, the NOS scores ranged from 7 to 9, indicating moderate to high methodological quality. The highest score (9) was reported in the studies by Wulandari (2015) and Harada (2024), reflecting a stronger design and reporting. In contrast, Eagan (2002), Mosquera (2014), Toerper (2014), and McCray (2018) scored 7, reflecting relative limitations, particularly in the comparability and outcome/exposure domains. Nevertheless, all the included studies met at least the minimum quality standards for inclusion in the final analysis.
Table 1: Quality Assessment of Included Studies
| Author | Year | Selection | Comparability | Outcome/Exposure | Total Score | Ref |
| Eagan et al. | (2002) | 3 | 1 | 3 | 7 | 13 |
| Askarian et al. | (2010) | 3 | 2 | 3 | 8 | 14 |
| Maroufi et al. | (2012) | 4 | 2 | 2 | 8 | 15 |
| Mosquera et al. | (2014) | 3 | 1 | 3 | 7 | 16 |
| Toerper et al. | (2014) | 3 | 1 | 3 | 7 | 17 |
| Fasola et al. | (2014) | 3 | 2 | 3 | 8 | 18 |
| Wulandari et al. | (2015) | 4 | 2 | 3 | 9 | 19 |
| Abbasi et al. | (2017) | 3 | 2 | 3 | 8 | 20 |
| McCray et al. | (2018) | 4 | 1 | 2 | 7 | 21 |
| Yamada et al. | (2020) | 3 | 2 | 3 | 8 | 22 |
| Yamada et al. | (2023) | 3 | 2 | 3 | 8 | 23 |
| Harada et al. | (2024) | 4 | 2 | 3 | 9 | 24 |
Table 2 presents the main characteristics of the 13 studies included in this systematic review. These studies were conducted in diverse countries, including Iran, Indonesia, Italy, Japan, Australia, Spain, Israel, and the United States. Various study designs, including cross-sectional, interventional, retrospective, and simulation-based, have been employed to evaluate waste minimization interventions in hospital and clinical settings. The types of healthcare waste assessed across the studies included pharmaceutical, infectious, chemical, radioactive, sharps, and food waste. This diversity reflects the wide range of challenges and strategies applied in healthcare waste management across middle- and high-income countries.
Table 2: Characteristics and Key Findings of Included Studies on Health Care Waste Minimization Strategies
| Ref | Country | Study design | Setting | Waste type(s) studied |
| 13 | USA | Case study | 9 hospitals and clinics | Chemical |
| 14 | Iran | Interventional (before–after) | Namazi Hospital (600 beds, 85% occupancy) | Infectious, non-infectious, and sharps |
| 15 | Iran | Descriptive cross-sectional | Public and private hospitals | Sharps, radioactive, chemical |
| 16 | Spain | Quasi-experimental | One specialty hospital | Pharmaceutical, sharps, radioactive, chemical |
| 17 | USA | Pre–and intervention with simulation | Children’s Hospital (205 beds) | Pharmaceutical |
| 18 | Italy | Retrospective interventional | Oncology ward, Udine University Hospital | Pharmaceutical |
| 19 | Indonesia | Descriptive cross-sectional | Public hospital | Infectious, pharmaceutical, pathological, sharps, chemical, radioactive |
| 20 | USA | Two-stage single-group intervention | One private hospital | Pharmaceutical |
| 21 | Australia | Retrospective comparative study | One public hospital | Food waste |
| 22 | Japan | Observational pre–post | Gifu University Hospital | Pharmaceutical |
| 23 | Japan | Retrospective comparative study | Two public hospitals | Pharmaceutical |
| 24 | Japan | Retrospective observational | Ashigaragami and Ogaki hospitals | Pharmaceutical |
Table 3 summarizes the interventions, outcome measures, key findings, and limitations reported in the 13 studies included in this review. A wide range of strategies have been applied in different healthcare settings to minimize medical waste. The findings indicate that educational and managerial interventions, such as the implementation of Total Quality Management (TQM) models, staff training, improvement of WHO guidelines, and awareness-raising sessions, led to significant reductions in both infectious and non-infectious waste, while also improving the quality of waste segregation 14-16. Pharmacy-related interventions, including adjustments in drug preparation frequency, the use of multi-dose vials, dose rounding, and prescription review by pharmacists, were highly effective in reducing pharmaceutical waste and achieving substantial cost savings 17, 18, 20, 22-24. These findings highlight the value of pharmacy bundles (integrated sets of clinical and managerial interventions) for optimizing drug utilization. Hospital nutrition interventions, such as redesigning food services and involving nutritionists, not only reduce food waste but also enhance patient satisfaction and lower dietary costs 21. Technological and environmental interventions, including the substitution of hazardous chemicals, limited reuse of certain equipment, and application of environmental impact assessment tools, have contributed to reductions in hazardous waste and improvements in staff safety 13, 19. Overall, this review suggests that multifaceted interventions, particularly the integration of educational, managerial, pharmaceutical, and nutritional strategies, are the most effective approaches for reducing waste volume and cost in hospitals. The use of multidimensional approaches and pharmacy bundles appears to yield sustainable and generalizable results.
Table 3: Summary of Interventions, Outcome Indicators, Key Findings, and Limitations of Included Studies
| Author | Intervention Category |
Targeted Waste |
Intervention / Strategy | Outcome Measurement Indicators | Key Findings | Limitations | Ref |
| Eagan et al. (2002) | Educational and Managerial Interventions / Technological and Environmental Interventions | Chemical | Use of the HCEPT tool for selecting low environmental impact products | - Amount of mercury removed (g) - Staff awareness level (questionnaire) - Continuity of tool usage in centers |
Removal of 1,084 g of mercury in 2 centers; increased staff awareness; continued use in 5 out of 9 centers | Small sample size, voluntary participation (selection bias), limited generalizability | 13 |
| Askarian et al. (2010) | Educational and Managerial Interventions | Infectious, Non-infectious | Implementation of TQM with FOCUS-PDCA model (waste redefinition, 10 training sessions, posters and brochures, container recoding) | - Waste weight (kg/bed/day) - % of infectious/non-infectious waste (pre/post) - Cost (USD) |
Reduction from 6.67 to 5.92 kg/bed/day; 26% reduction in infectious waste; 26% cost savings | Single hospital; one-month follow-up; sustainability or infection assessment not conducted | 14 |
| Maroufi et al. (2012) | Educational and Managerial Interventions | Infectious, Chemical | Implementation of the WHO waste management guidelines by staff | - Staff awareness level (questionnaire) - Waste weight (kg/ward/day) |
Significant improvement in awareness; reduced waste generation in some wards | Self-reported data; limited generalizability | 15 |
| Mosquera et al. (2014) | Educational and Managerial Interventions / Technological and Environmental Interventions | Pharmaceutical, Infectious, Chemical | Educational sessions on segregation of healthcare waste (HCW) | Waste volume, financial savings, segregation quality | 6.2% reduction in waste volume; €125,205 saved; improved segregation | Single hospital; short follow-up period | 16 |
| Toerper et al. (2014) | Pharmaceutical Interventions | Pharmaceutical | Change from once to three times daily preparation of injectable drugs; simulation of 108 batching schedules using an algorithm | Drug waste rate, annual savings | Waste reduced from 28.7% to 19.7%; annual savings of $183,380; best results at ≥2 preparations/day. | Single hospital; simulation limitations; logistical and workforce effects not assessed | 17 |
| Fasola et al. (2014) | Pharmaceutical Interventions / Educational and Managerial Interventions | Pharmaceutical | Protocol from Jan 2006: weekly scheduling of drug administration, multi-dose vials with stability up to 24h, dose rounding ±5%, optimal vial size selection | Annual/monthly pharmaceutical waste cost, trends in expensive drug use, and waste | 45% reduction in pharmaceutical waste cost; ~30% reduction in high-cost drug expenses | Patient clinical outcomes not assessed; market-dependent; limited generalizability | 18 |
| Wulandari et al. (2015) | Educational and Managerial Interventions / Technological and Environmental Interventions | Infectious, Pharmaceutical, Chemical | Segregation, cleaning, preventive maintenance; clean technology (esp. radiology); replacement of disinfectants (Renalin vs. formalin); limited reuse (dialysis bottles, glassware) | Waste generation (kg/bed/day) | 0.9 kg/bed/day with 64% occupancy; effective reuse in dialysis; reduced hazardous waste via targeted purchasing | No recycling; limited reuse; single hospital; legal/economic constraints; no long-term evaluation | 19 |
| Abbasi et al. (2017) | Pharmaceutical Interventions | Pharmaceutical | Change in sterile compounding batching frequency (2x → 4x/day) with 8-day washout | Number of wasted CSPs and cost | CSPs reduced from 97 to 83; decrease in low-cost drugs, increase in high-cost drugs; cost savings for low-cost drugs | Single-center, non-randomized, 7-day study, only drug/solvent costs included, staff costs not assessed. | 20 |
| McCray et al. (2018) | Hospital Nutrition Interventions | Food | Implementation of redesigned food service model (RS) focusing on patient needs | Food intake, plate waste, patient satisfaction, and food cost | Plate waste decreased from 30% to 17%; patient satisfaction increased from 75% to 98%; food cost ↓ 28% | Non-randomized design; limited reporting of model details | 21 |
| Yamada et al. (2020) | Pharmaceutical Interventions | Pharmaceutical | Pharmacist-based eligibility review, dose reduction, drug discontinuation before preparation | Drug discard rate, discard cost | Discard rate from 0.367% to 0.032%; cost ↓ from $18,562 to $3,622 | Single-center, short-term analysis, limited generalizability | 22 |
| Yamada et al. (2023) | Pharmaceutical Interventions | Pharmaceutical | Added infection status check (fever ≥ 37.5°C, elevated CRP/WBC) to pharmacist checklist before preparation | Drug discard rate/number; reasons; cost impact | Discard rate from 0.288% to 0.095% (P=0.013); infection-related discards from 11 to 1; improved efficiency. | Retrospective design; single hospital; no direct patient-level outcomes | 23 |
| Harada et al. (2024) | Pharmaceutical Interventions | Pharmaceutical | Evaluation of DVO (dose vial optimization) and DR (dose rounding) methods | Drug waste and cost savings (DVO vs DR) | DR eliminated gemcitabine waste in Ogaki hospital and leucovorin in both hospitals; overall, DR was more effective | Two hospitals only; one-year study; results may not generalize to all anticancer drugs/centers | 24 |
Discussion
This study aimed to identify the most effective strategies for minimizing healthcare waste and enhancing its management. Our review is the first to highlight and synthesize evidence on pharmacy bundles (including dose rounding, vial optimization, batching frequency, and pharmacist-led review) and hospital food service redesign as high-impact waste-minimization strategies. Our findings highlighted that the highest-impact intervention was focused on staff training coupled with a systematic reorganization of waste segregation procedures. This intervention does not require substantial financial investment and is particularly effective in reducing infectious waste and improving waste segregation management. Its main limitation lies in its strong dependence on continuous training and ongoing monitoring of staff behavior, as its effectiveness diminishes if attention and follow-up are reduced. Redesigning hospital food services was identified as another highly impactful strategy. This intervention not only reduced food waste but also improved patient satisfaction and led to substantial financial savings. However, it requires moderate upfront investment and structural changes in menus, ordering systems, and the presence of nutrition specialists in schools. Despite these initial costs, the return on investment becomes evident within a relatively short timeframe, highlighting its importance.
The third-ranked intervention involves the substitution of hazardous substances and the adoption of clean technologies, such as the use of Renalin instead of formalin and the implementation of digital imaging systems. These interventions are particularly relevant from an environmental sustainability perspective, as they reduce chemical and hazardous waste and enhance the safety of the staff. However, their installation costs are relatively high, and the financial benefits vary depending on hospital-specific conditions.
Finally, green procurement tools, such as HCEPT, represent a complementary strategy. Their impact is largely indirect and becomes apparent over the long term by eliminating hazardous substances and fostering a culture of sustainability within healthcare organizations. Although the implementation costs are relatively low, immediate financial returns are limited. Thus, this approach is best viewed as part of a broader institutional waste management program.
Educational and managerial interventions
For example, Mosquera (2014) in Spain demonstrated that targeted staff training in healthcare waste segregation reduced waste volume by 6.2%, generated substantial economic savings (> €125,000), and improved segregation quality 16. Similarly, Askarian et al.(2010) in Iran reported that staff training, policy revision, and redefinition of infectious and non-infectious waste categories led to a reduction of 0.75 kg of waste per bed per day and a 26% cost reduction 14.
Pharmacy-related interventions
Abbasi (2017) and Toerper (2014) in the United States showed that altering the drug preparation frequency significantly reduced pharmaceutical waste. Reducing the frequency of sterile compounding from four to two times daily lowered drug wastage and achieved notable cost savings. Simulation-based models in Toerper’s study demonstrated a decrease in waste rates from 28.7% to 19.7% and an annual saving of USD 183,380 17, 20. Fasola (2014) in Italy found that the use of multi-dose vials, ±5% dose rounding, optimized vial selection, and weekly scheduling of chemotherapy administration reduced pharmaceutical waste costs by approximately 45% 18.
In Japan, a pharmacist-led protocol introduced in 2020, which included reviewing patient conditions and the likelihood of dose reduction or treatment discontinuation before preparation, reduced drug discard rates from 0.367% to 0.032% and substantially reduced costs 22. Yamada (2023) further demonstrated that adding infection markers (fever, CRP, WBC) to pharmacists’ checklists significantly lowered drug wastage (from 0.288% to 0.095%) 23. Harada (2024) compared “dose vial optimization (DVO)” and “dose rounding (DR)” in two Japanese hospitals and found that DR was more effective, even eliminating waste for some drugs while reducing costs across different settings 24.
Collectively, these findings highlight that pharmacy bundles—integrating DR, DVO, preparation scheduling, and pharmacist-led clinical review–are the most cost-effective and rapidly impactful interventions. They require minimal additional investment, relying primarily on protocol revisions, staff training, and interdisciplinary collaboration.
Technological and environmental interventions
Studies such as Wulandari (2015) and Askarian (2010) emphasize clean technology adoption, hazardous material substitution, and preventive maintenance. Key examples include replacing formalin with Renalin, introducing digital imaging, and returning expired drugs to the distributors. These measures reduced medical waste generation to approximately 0.9 kg per bed per day 14, 19. Limited reuse practices, such as reusing dialysis containers or glass bottles, have been noted in Indonesia; however, challenges such as regulatory barriers, contamination risks, quality control, and cost constraints hinder wider adoption 19.
Hospital nutrition interventions
McCray (2018) focused on food waste management by hiring nutritionists, analyzing menus, training staff, and redesigning food services. These interventions significantly reduced plate waste (from 30% to 17%), generated cost savings, and enhanced patient satisfaction 21.
Limitations of Current Evidence
Despite these encouraging results, several limitations were common across the studies. Most interventions were conducted in single-center settings with retrospective or nonrandomized designs. Most focused primarily on environmental and economic outcomes, with little attention to patient-centered clinical endpoints, staff safety, or long-term sustainability. Follow-up durations were often short, making it difficult to assess whether the interventions remained effective over time. As highlighted by Ali et al. (2017), waste management interventions in healthcare are often unsustainable unless embedded within organizational and cultural structures 25.
Implications for Practice
The findings of this review highlight several practical strategies for improving healthcare waste management in developing countries. Education and capacity building through structured staff training and the development of updated internal protocols can significantly enhance segregation practices and reduce the costs. In the area of pharmacy management, pharmacist-led protocols, dose rounding, vial optimization, and preparation scheduling have proven to be among the most effective interventions, leading to reduced pharmaceutical waste and rapid financial savings. The adoption of clean technologies, such as substituting hazardous substances like Renalin for formalin and using digital imaging, contributes to reducing hazardous waste and improving occupational safety. Hospital food management strategies, including menu redesign, greater involvement of nutritionists, and restructuring food services, help minimize food waste and simultaneously improve patient satisfaction. Finally, green procurement initiatives supported by tools such as the HCEPT provide an environmentally sustainable framework that fosters long-term cultural and systemic change.
Conclusion
This review demonstrates that the most effective and economically viable approach to hospital waste reduction is the implementation of pharmacy bundles consisting of four core components: dose rounding (DR), dose/vial optimization (DVO), scheduling of sterile preparation, and pharmacist-led patient condition review using clinical checklists. Together, these strategies offer proven cost savings, straightforward implementation, and direct reduction of pharmaceutical waste. Evidence shows that this approach can achieve substantial percentage reductions in drug discard, annual savings in the six-figure range (USD/EUR), and even complete elimination of waste for certain medications.
Acknowledgments
The authors would like to gratefully acknowledge the Research Deputy of Shahid Sadoughi University of Medical Sciences, Yazd.
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This study was funded by the Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Ethical Considerations
The authors obtained permission from the Ethics Committee of the Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Code of Ethics
The present study was approved by the code of ethics IR.SSU.SPH.REC.1403.037 of Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Ethical approval
The present study was approved by the code of ethics IR.SSU.SPH.REC.1403.037 of Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Data availability statement
Supporting data are available from the corresponding authors upon reasonable request.
Authors contributions
All authors contributed to the conception and design of this study. Material preparation, data collection, and analysis were performed by all the authors. The first draft of the manuscript was written by L.N. and A.D., and all authors commented on the previous versions of the manuscript. All the authors have read and approved the final manuscript. Conceptualization: L.N., A.D., H.N., and M.M.; Methodology: L.N., A.D., H.N., and M.M.Formal analysis and investigation by L.N. and A.D.Writing the original draft was prepared by L.N., A.D., and H.N.Writing, review, and editing by all authors.
Competing interests
The authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this study.
This is an Open-Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt, and build upon this work for commercial use.
References
1. Kaposi A, Nagy A, Gomori G, et al. Analysis of healthcare waste and factors affecting the amount of hazardous healthcare waste in a university hospital. J Mater Cycles Waste Manag. 2024;26(2):1169-80.
2. Patel JN, Upadhyay SK, Rajbhandari A, et al. Knowledge about handling hazardous materials as factors associated with adherence to healthcare waste management practices among waste handlers at government district hospitals of Madhesh province, Nepal: a quantitative-qualitative methods study. PLOS Glob Public Health. 2024;4(12):e0002028.
3. Tadesse ML. Healthcare waste generation and quantification in public health centres in Addis Ababa, Ethiopia. PLoS One. 2024;19(2): e0295165.
4. Singh N, Ogunseitan OA, Tang Y. Medical waste: current challenges and future opportunities for sustainable management. Crit Rev Environ Sci Technol. 2022;52(11):2000-22.
5. Cheng Y, Sung F, Yang Y, et al. Medical waste production at hospitals and associated factors. Waste Management. 2009;29(1):440-4.
6. Haylie GM, Genet M, Worede EA, et al. Hazardous waste management practices among healthcare workers in Gondar City, Ethiopia. Sci Rep. 2025;15(1):18647.
7. Ananth AP, Prashanthini V, Visvanathan C. Healthcare waste management in Asia. Waste Management. 2010;30(1):154-61.
8. Mostaghimi K, Behnamian J. Waste minimization towards waste management and cleaner production strategies: a literature review. Environ Dev Sustain. 2023;25(11):12119-66.
9. Torkayesh A, Vandchali H, Tirkolaee E. Multi-objective optimization for healthcare waste management network design with sustainability perspective. Sustainability. 2021; 13 (15): 1-17.
10. Sasikumar A, Acharya P, Nair M, et al. Applying lean six sigma for waste reduction in a bias tyre manufacturing environment. Cogent Business & Management. 2023;10(2):2228551.
11. Mark Vrabel M, editor. Preferred reporting items for systematic reviews and meta-analyses. InOncology nursing forum 2015;42(5):552. Oncology Nursing Society.
12. Luchini C, Stubbs B, Solmi M, et al. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Metaanal. 2017;5(4):80-4.
13. Eagan PD, Kaiser B. Can environmental purchasing reduce mercury in US health care? Environ Health Perspect. 2002;110(9):847-51.
14. Askarian M, Heidarpoor P, Assadian O. A total quality management approach to healthcare waste management in Namazi Hospital, Iran. Waste Management. 2010;30(11):2321-6.
15. Maroufi M, Javadi M, Karimi S. Function of nurses and other staff to minimize hospital waste in selected hospitals in Isfahan. Iran J Nurs Midwifery Res. 2012;17(6):445-50.
16. Mosquera M, Andrés-Prado MJ, Rodríguez-Caravaca G, et al. Evaluation of an education and training intervention to reduce health care waste in a tertiary hospital in Spain. Am J Infect Control. 2014;42(8):894-7.
17. Toerper MF, Veltri MA, Hamrock E, et al. Medication waste reduction in pediatric pharmacy batch processes. J Pediatr Pharmacol Ther. 2014;19(2):111-7.
18. Fasola G, Aprile G, Marini L, et al. Drug waste minimization as an effective strategy of cost-containment in oncology. BMC Health Serv Res. 2014;14(1):57.
19. Wulandari P, Kusnoputranto H. Medical waste management and minimization efforts at public hospital. case study: public hospital in East Jakarta, Indonesia. Kes Mas: Jurnal Fakultas Kesehatan Masyarakat Universitas Ahmad Daulan. 2015;9(2):25028.
20. Abbasi G, Gay E. Impact of sterile compounding batch frequency on pharmaceutical waste. Hospital Pharmacy. 2017;52(1):60-4.
21. McCray S, Maunder K, Barsha L, et al. Room service in a public hospital improves nutritional intake and increases patient satisfaction while decreasing food waste and cost. Journal of Human Nutrition and Dietetics. 2018;31(6):734-41.
22. Yamada H, Kobayashi R, Shimizu S, et al. Implementation of a standardised pharmacist check of medical orders prior to preparation of anticancer drugs to reduce drug wastage. Int J Clin Pract. 2020; 74(4): e13464.
23. Yamada H, Yamada Y, Iihara H, et al. A pharmacist check of patients’ infection-related condition prior to drug preparation reduces anticancer drug wastage after mixing: a retrospective study. J Pharm Policy Pract. 2023;16(1):5.
24. Harada T, Usami E, Aso T, et al. Comparison of dose rounding and drug vial optimization for reducing anticancer drug waste. Journal of Oncology Pharmacy Practice. 2024: 10781552251341567.
25. Ali M, Wang W, Chaudhry N, et al. Hospital waste management in developing countries: a mini review. Waste Manag Res. 2017;35(6):581-92.
This study aimed to identify the most effective strategies for minimizing healthcare waste and enhancing its management. Our review is the first to highlight and synthesize evidence on pharmacy bundles (including dose rounding, vial optimization, batching frequency, and pharmacist-led review) and hospital food service redesign as high-impact waste-minimization strategies. Our findings highlighted that the highest-impact intervention was focused on staff training coupled with a systematic reorganization of waste segregation procedures. This intervention does not require substantial financial investment and is particularly effective in reducing infectious waste and improving waste segregation management. Its main limitation lies in its strong dependence on continuous training and ongoing monitoring of staff behavior, as its effectiveness diminishes if attention and follow-up are reduced. Redesigning hospital food services was identified as another highly impactful strategy. This intervention not only reduced food waste but also improved patient satisfaction and led to substantial financial savings. However, it requires moderate upfront investment and structural changes in menus, ordering systems, and the presence of nutrition specialists in schools. Despite these initial costs, the return on investment becomes evident within a relatively short timeframe, highlighting its importance.
The third-ranked intervention involves the substitution of hazardous substances and the adoption of clean technologies, such as the use of Renalin instead of formalin and the implementation of digital imaging systems. These interventions are particularly relevant from an environmental sustainability perspective, as they reduce chemical and hazardous waste and enhance the safety of the staff. However, their installation costs are relatively high, and the financial benefits vary depending on hospital-specific conditions.
Finally, green procurement tools, such as HCEPT, represent a complementary strategy. Their impact is largely indirect and becomes apparent over the long term by eliminating hazardous substances and fostering a culture of sustainability within healthcare organizations. Although the implementation costs are relatively low, immediate financial returns are limited. Thus, this approach is best viewed as part of a broader institutional waste management program.
Educational and managerial interventions
For example, Mosquera (2014) in Spain demonstrated that targeted staff training in healthcare waste segregation reduced waste volume by 6.2%, generated substantial economic savings (> €125,000), and improved segregation quality 16. Similarly, Askarian et al.(2010) in Iran reported that staff training, policy revision, and redefinition of infectious and non-infectious waste categories led to a reduction of 0.75 kg of waste per bed per day and a 26% cost reduction 14.
Pharmacy-related interventions
Abbasi (2017) and Toerper (2014) in the United States showed that altering the drug preparation frequency significantly reduced pharmaceutical waste. Reducing the frequency of sterile compounding from four to two times daily lowered drug wastage and achieved notable cost savings. Simulation-based models in Toerper’s study demonstrated a decrease in waste rates from 28.7% to 19.7% and an annual saving of USD 183,380 17, 20. Fasola (2014) in Italy found that the use of multi-dose vials, ±5% dose rounding, optimized vial selection, and weekly scheduling of chemotherapy administration reduced pharmaceutical waste costs by approximately 45% 18.
In Japan, a pharmacist-led protocol introduced in 2020, which included reviewing patient conditions and the likelihood of dose reduction or treatment discontinuation before preparation, reduced drug discard rates from 0.367% to 0.032% and substantially reduced costs 22. Yamada (2023) further demonstrated that adding infection markers (fever, CRP, WBC) to pharmacists’ checklists significantly lowered drug wastage (from 0.288% to 0.095%) 23. Harada (2024) compared “dose vial optimization (DVO)” and “dose rounding (DR)” in two Japanese hospitals and found that DR was more effective, even eliminating waste for some drugs while reducing costs across different settings 24.
Collectively, these findings highlight that pharmacy bundles—integrating DR, DVO, preparation scheduling, and pharmacist-led clinical review–are the most cost-effective and rapidly impactful interventions. They require minimal additional investment, relying primarily on protocol revisions, staff training, and interdisciplinary collaboration.
Technological and environmental interventions
Studies such as Wulandari (2015) and Askarian (2010) emphasize clean technology adoption, hazardous material substitution, and preventive maintenance. Key examples include replacing formalin with Renalin, introducing digital imaging, and returning expired drugs to the distributors. These measures reduced medical waste generation to approximately 0.9 kg per bed per day 14, 19. Limited reuse practices, such as reusing dialysis containers or glass bottles, have been noted in Indonesia; however, challenges such as regulatory barriers, contamination risks, quality control, and cost constraints hinder wider adoption 19.
Hospital nutrition interventions
McCray (2018) focused on food waste management by hiring nutritionists, analyzing menus, training staff, and redesigning food services. These interventions significantly reduced plate waste (from 30% to 17%), generated cost savings, and enhanced patient satisfaction 21.
Limitations of Current Evidence
Despite these encouraging results, several limitations were common across the studies. Most interventions were conducted in single-center settings with retrospective or nonrandomized designs. Most focused primarily on environmental and economic outcomes, with little attention to patient-centered clinical endpoints, staff safety, or long-term sustainability. Follow-up durations were often short, making it difficult to assess whether the interventions remained effective over time. As highlighted by Ali et al. (2017), waste management interventions in healthcare are often unsustainable unless embedded within organizational and cultural structures 25.
Implications for Practice
The findings of this review highlight several practical strategies for improving healthcare waste management in developing countries. Education and capacity building through structured staff training and the development of updated internal protocols can significantly enhance segregation practices and reduce the costs. In the area of pharmacy management, pharmacist-led protocols, dose rounding, vial optimization, and preparation scheduling have proven to be among the most effective interventions, leading to reduced pharmaceutical waste and rapid financial savings. The adoption of clean technologies, such as substituting hazardous substances like Renalin for formalin and using digital imaging, contributes to reducing hazardous waste and improving occupational safety. Hospital food management strategies, including menu redesign, greater involvement of nutritionists, and restructuring food services, help minimize food waste and simultaneously improve patient satisfaction. Finally, green procurement initiatives supported by tools such as the HCEPT provide an environmentally sustainable framework that fosters long-term cultural and systemic change.
Conclusion
This review demonstrates that the most effective and economically viable approach to hospital waste reduction is the implementation of pharmacy bundles consisting of four core components: dose rounding (DR), dose/vial optimization (DVO), scheduling of sterile preparation, and pharmacist-led patient condition review using clinical checklists. Together, these strategies offer proven cost savings, straightforward implementation, and direct reduction of pharmaceutical waste. Evidence shows that this approach can achieve substantial percentage reductions in drug discard, annual savings in the six-figure range (USD/EUR), and even complete elimination of waste for certain medications.
Acknowledgments
The authors would like to gratefully acknowledge the Research Deputy of Shahid Sadoughi University of Medical Sciences, Yazd.
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This study was funded by the Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Ethical Considerations
The authors obtained permission from the Ethics Committee of the Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Code of Ethics
The present study was approved by the code of ethics IR.SSU.SPH.REC.1403.037 of Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Ethical approval
The present study was approved by the code of ethics IR.SSU.SPH.REC.1403.037 of Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Data availability statement
Supporting data are available from the corresponding authors upon reasonable request.
Authors contributions
All authors contributed to the conception and design of this study. Material preparation, data collection, and analysis were performed by all the authors. The first draft of the manuscript was written by L.N. and A.D., and all authors commented on the previous versions of the manuscript. All the authors have read and approved the final manuscript. Conceptualization: L.N., A.D., H.N., and M.M.; Methodology: L.N., A.D., H.N., and M.M.Formal analysis and investigation by L.N. and A.D.Writing the original draft was prepared by L.N., A.D., and H.N.Writing, review, and editing by all authors.
Competing interests
The authors declare that they have no competing financial interests or personal relationships that could have influenced the work reported in this study.
This is an Open-Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt, and build upon this work for commercial use.
References
1. Kaposi A, Nagy A, Gomori G, et al. Analysis of healthcare waste and factors affecting the amount of hazardous healthcare waste in a university hospital. J Mater Cycles Waste Manag. 2024;26(2):1169-80.
2. Patel JN, Upadhyay SK, Rajbhandari A, et al. Knowledge about handling hazardous materials as factors associated with adherence to healthcare waste management practices among waste handlers at government district hospitals of Madhesh province, Nepal: a quantitative-qualitative methods study. PLOS Glob Public Health. 2024;4(12):e0002028.
3. Tadesse ML. Healthcare waste generation and quantification in public health centres in Addis Ababa, Ethiopia. PLoS One. 2024;19(2): e0295165.
4. Singh N, Ogunseitan OA, Tang Y. Medical waste: current challenges and future opportunities for sustainable management. Crit Rev Environ Sci Technol. 2022;52(11):2000-22.
5. Cheng Y, Sung F, Yang Y, et al. Medical waste production at hospitals and associated factors. Waste Management. 2009;29(1):440-4.
6. Haylie GM, Genet M, Worede EA, et al. Hazardous waste management practices among healthcare workers in Gondar City, Ethiopia. Sci Rep. 2025;15(1):18647.
7. Ananth AP, Prashanthini V, Visvanathan C. Healthcare waste management in Asia. Waste Management. 2010;30(1):154-61.
8. Mostaghimi K, Behnamian J. Waste minimization towards waste management and cleaner production strategies: a literature review. Environ Dev Sustain. 2023;25(11):12119-66.
9. Torkayesh A, Vandchali H, Tirkolaee E. Multi-objective optimization for healthcare waste management network design with sustainability perspective. Sustainability. 2021; 13 (15): 1-17.
10. Sasikumar A, Acharya P, Nair M, et al. Applying lean six sigma for waste reduction in a bias tyre manufacturing environment. Cogent Business & Management. 2023;10(2):2228551.
11. Mark Vrabel M, editor. Preferred reporting items for systematic reviews and meta-analyses. InOncology nursing forum 2015;42(5):552. Oncology Nursing Society.
12. Luchini C, Stubbs B, Solmi M, et al. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Metaanal. 2017;5(4):80-4.
13. Eagan PD, Kaiser B. Can environmental purchasing reduce mercury in US health care? Environ Health Perspect. 2002;110(9):847-51.
14. Askarian M, Heidarpoor P, Assadian O. A total quality management approach to healthcare waste management in Namazi Hospital, Iran. Waste Management. 2010;30(11):2321-6.
15. Maroufi M, Javadi M, Karimi S. Function of nurses and other staff to minimize hospital waste in selected hospitals in Isfahan. Iran J Nurs Midwifery Res. 2012;17(6):445-50.
16. Mosquera M, Andrés-Prado MJ, Rodríguez-Caravaca G, et al. Evaluation of an education and training intervention to reduce health care waste in a tertiary hospital in Spain. Am J Infect Control. 2014;42(8):894-7.
17. Toerper MF, Veltri MA, Hamrock E, et al. Medication waste reduction in pediatric pharmacy batch processes. J Pediatr Pharmacol Ther. 2014;19(2):111-7.
18. Fasola G, Aprile G, Marini L, et al. Drug waste minimization as an effective strategy of cost-containment in oncology. BMC Health Serv Res. 2014;14(1):57.
19. Wulandari P, Kusnoputranto H. Medical waste management and minimization efforts at public hospital. case study: public hospital in East Jakarta, Indonesia. Kes Mas: Jurnal Fakultas Kesehatan Masyarakat Universitas Ahmad Daulan. 2015;9(2):25028.
20. Abbasi G, Gay E. Impact of sterile compounding batch frequency on pharmaceutical waste. Hospital Pharmacy. 2017;52(1):60-4.
21. McCray S, Maunder K, Barsha L, et al. Room service in a public hospital improves nutritional intake and increases patient satisfaction while decreasing food waste and cost. Journal of Human Nutrition and Dietetics. 2018;31(6):734-41.
22. Yamada H, Kobayashi R, Shimizu S, et al. Implementation of a standardised pharmacist check of medical orders prior to preparation of anticancer drugs to reduce drug wastage. Int J Clin Pract. 2020; 74(4): e13464.
23. Yamada H, Yamada Y, Iihara H, et al. A pharmacist check of patients’ infection-related condition prior to drug preparation reduces anticancer drug wastage after mixing: a retrospective study. J Pharm Policy Pract. 2023;16(1):5.
24. Harada T, Usami E, Aso T, et al. Comparison of dose rounding and drug vial optimization for reducing anticancer drug waste. Journal of Oncology Pharmacy Practice. 2024: 10781552251341567.
25. Ali M, Wang W, Chaudhry N, et al. Hospital waste management in developing countries: a mini review. Waste Manag Res. 2017;35(6):581-92.
Type of Study: Systematic Review |
Subject:
Solid remediation and wastes
Received: 2025/10/23 | Accepted: 2026/01/20 | Published: 2026/03/23
Received: 2025/10/23 | Accepted: 2026/01/20 | Published: 2026/03/23
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
